Vertebroplasty and kyphoplasty are minimally invasive surgeries that play a critical role in the management of back pain stemming from vertebral compression fractures. These procedures are generally considered when conservative treatment options, such as pain medications and physical therapy, do not relieve pain from fractures commonly caused by osteoporosis. We understand that persistent pain can significantly impact quality of life, and these treatments aim to provide pain relief and stabilize the fracture.
Compression fractures can lead to a decrease in mobility, function, and wellbeing. In vertebroplasty, medical-grade bone cement is injected directly into the damaged vertebrae, quickly providing stability and pain relief. Kyphoplasty follows a similar principle, but initially involves the insertion of a balloon to create a cavity for the cement, potentially restoring some of the vertebral height. These procedures typically have a high success rate, offering an interventional solution that can drastically improve our patient’s pain and functionality.
Key Takeaways
- Vertebroplasty and kyphoplasty can effectively treat back pain from osteoporotic compression fractures.
- These minimally invasive procedures stabilize the spine and can alleviate pain rapidly.
- Creating a treatment plan for spinal fractures often includes preoperative, operative, and postoperative considerations to ensure optimal recovery and efficacy.
Understanding Vertebroplasty and Kyphoplasty
In this section, we will explore the specifics of vertebroplasty and kyphoplasty—two minimally invasive procedures that have transformed the treatment of vertebral compression fractures. We’ll detail what each procedure entails and how they have developed over time.
Definitions and Differences
Vertebroplasty is a surgical procedure in which a special bone cement, known as polymethylmethacrylate (PMMA), is injected directly into the collapsed or fractured vertebra. This cement injection stabilizes the bone and provides significant pain relief.
Kyphoplasty, while similar to vertebroplasty, involves an additional step before cement injection. A balloon-like device is first inserted and inflated to create space within the vertebra, aiming to restore some of the lost vertebral height. Only after this space is created is the PMMA applied.
Despite their similarities, the key differences lie in the approach to restoring vertebral structure and the risk of cement leakage, with kyphoplasty potentially offering more control over the cement application.
Historical Development
The inception of vertebroplasty can be traced back to France in the 1980s, where it was initially used to treat vertebral angiomas. Due to its success in stabilizing and pain relief, the technique was adapted to address osteoporotic fractures.
Kyphoplasty was introduced as a variation of vertebroplasty in the late 1990s, with the goal of correcting spinal deformities resulting from compression fractures. Since then, both procedures have undergone numerous refinements and have proven to be effective treatment modalities for patients who do not respond to traditional medical management of compression fractures.
Indications and Contraindications
In the management of vertebral fractures, percutaneous vertebroplasty and kyphoplasty are significant procedures with specific eligibilities and limitations. We will explore the conditions under which these procedures are recommended and the constraints that may prohibit their use.

Eligibility for Procedures
Indications:
- Osteoporosis: Patients with painful osteoporotic compression fractures are primary candidates.
- Tumor: The procedures are indicated for vertebral compression fractures due to a tumor or cancer lesion weakening the spine.
- Pain Relief: Individuals with vertebral fractures experiencing debilitating pain, not responding to conservative treatment, may benefit.
Contraindications:
- Asymptomatic Fractures: Fractures that do not cause pain are not typically treated with these procedures.
- Bleeding Disorders: Patients on blood thinners or those with coagulation disorders are at increased risk and may not be eligible.
Risks and Limitations
Risks:
- There exists the potential risk of cement leakage, which may lead to neurological complications.
- In rare cases, procedures can introduce or exacerbate infection.
Limitations:
- If a vertebra has healed significantly or if a fracture is very old, the benefits of vertebroplasty or kyphoplasty may be reduced.
- Patients with allergic reactions to materials used in the procedure, such as surgical polymethylmethacrylate (PMMA) cement, must avoid it.
In summary, these procedures offer a therapeutic option with a clear set of indications, particularly beneficial for those suffering from vertebral fractures due to osteoporosis or malignancy. Yet, risks and patient-specific contraindications must be carefully weighed before proceeding.
Preoperative Considerations
Before we proceed with vertebroplasty or kyphoplasty, it is crucial that we conduct thorough patient assessments and ensure meticulous preparation for surgery. Doing so maximizes patient safety and optimizes the potential for a successful outcome.

Patient Assessment
We begin by evaluating the patient’s medical history, focusing on any recent illnesses or known allergies that could affect the procedure. Blood tests are essential to check for any issues that could complicate anesthesia or postoperative healing. We rely on magnetic resonance imaging (MRI) or computed tomography (CT) scans to confirm the diagnosis of vertebral compression fractures and to visualize the anatomy we will be addressing during the procedure. This imaging data allows us to plan the specifics of the intervention with precision.
Preparation for Surgery
Once we have assessed the patient, we ensure that preoperative instructions are clearly communicated. Crucial instructions include:
- Fasting protocols: No food or drink after midnight the day prior to the procedure.
- Medication guidelines: We review and modify the patient’s medications as required, especially any that may affect blood clotting or interact with anesthesia.
- Information on the procedure: We explain the steps involved in vertebroplasty/kyphoplasty, potential risks, and expected outcomes.
Finally, we confirm the surgical time and provide the patient with the necessary information on when to arrive at the hospital or surgical center.
Surgical Techniques

In our discussion, we’ll concentrate on the specific processes involved in vertebroplasty and kyphoplasty, two minimally invasive surgeries that are utilized to repair compression fractures in the vertebrae.
Vertebroplasty Procedure
In vertebroplasty, we make use of a needle to introduce a special cement mixture into the collapsed vertebra. The initial step settles on the correct patient positioning which allows us optimal access to the fractured site. Under fluoroscopy—a type of real-time X-ray—precision is crucial as we guide the needle into the vertebral body. After confirming the needle’s placement, we carefully inject the cement. The cement stabilizes the fracture and provides rapid pain relief.
This technique may be performed under local sedation or general anesthesia, depending on the patient’s condition and our assessment. As surgeons, we must ensure that the cement does not leak outside of the vertebral body which could potentially lead to complications.
Kyphoplasty Procedure
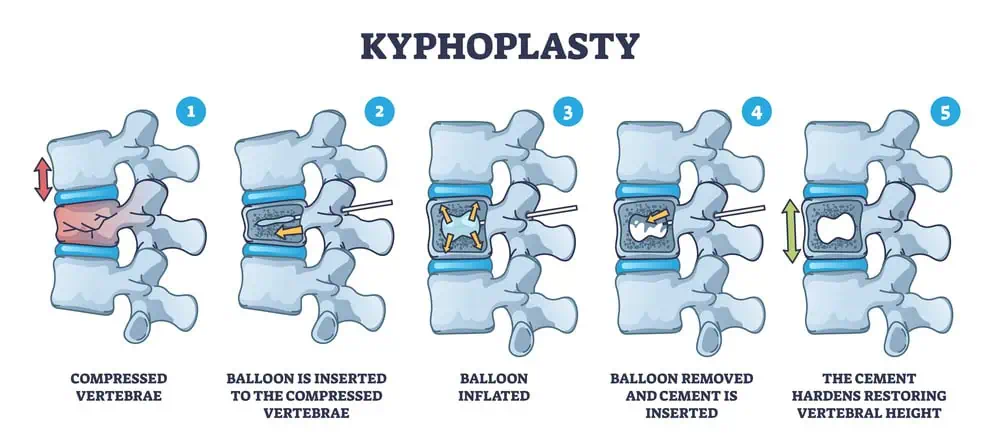
Kyphoplasty follows a similar pathway to vertebroplasty with a key addition. After we position our patient and gain access to the vertebra using a trocar, a balloon is inserted and then inflated to create a space within the fractured bone. This step aims to restore some of the lost vertebral height and correct the deformity.
Once the cavity is created, we deflate and remove the balloon, only to replace the void with cement. This reinforces the bone structure and alleviates pain. The precise delivery of the cement is monitored by fluoroscopy to ensure optimal filling and avoid spillage. As with vertebroplasty, kyphoplasty can be done under either local sedation or general anesthesia, based on our judgement and the individual’s medical status.
Postoperative Care and Recovery

Following a vertebroplasty or kyphoplasty procedure, we focus on ensuring effective pain relief while facilitating a smooth recovery. Our attention is directed towards immediate aftercare including wound management and early activity, as well as guiding patients through the rehabilitation phase with physical therapy tailored to their needs.
Immediate Aftercare
Immediately post-operation, we ensure the incision site is protected with a bandage and provide instructions on how to care for it. It’s common for patients to experience some soreness, but pain medication is administered to manage discomfort. We emphasize the importance of monitoring for any signs of infection or unexpected changes around the incision. Patients are generally able to walk within hours after the surgery and are often discharged the same day.
- Medication: Prescribed as needed for pain relief.
- Activity: Encouraged to move but to avoid heavy lifting or strenuous activities.
- Incision Care: Instructed to keep the area clean and dry; watch for signs of infection.
Rehabilitation and Physical Therapy
We introduce a rehabilitation plan to promote healing and restore mobility, which will often include physical therapy sessions. The goal of these sessions is not only to provide pain relief but also to strengthen the back muscles and improve posture to support the spine.
- Physical Therapy: Begins within a few weeks post-surgery.
- Strengthening: Targeted exercises to support the spine.
- Guidance: Ongoing support to ensure correct movement techniques.
Each patient’s recovery and therapy program is personalized, taking into account their specific condition and overall health.
Outcomes and Efficacy

In our assessment of vertebroplasty and kyphoplasty, we prioritize understanding both procedures’ effectiveness in managing pain and their long-term impact, including potential complications.
Pain Management Outcomes
We’ve found that both vertebroplasty and kyphoplasty are primarily utilized to provide pain relief following vertebral compression fractures. Pain reduction is typically rapid post-procedure, significantly improving patients’ quality of life by restoring mobility and reducing reliance on analgesics. In addition, both procedures aim to stabilize the fracture by injecting bone cement into the vertebral body, which often alleviates pain associated with the fracture.
Long-Term Effects and Complications
Our long-term analysis shows that while these procedures can offer sustained pain relief, they are not devoid of risks. Complications can include cement leakage, which, although infrequent, may lead to adverse effects if it enters the epidural space or vascular system. Moreover, there’s a discussion about whether these procedures could potentially lead to the development of new fractures in adjacent vertebrae. We must also monitor the progression of kyphosis, especially when the structural integrity of the spine is of concern.
By tackling these aspects, our goal is to provide a comprehensive understanding of what patients might expect with vertebroplasty and kyphoplasty, emphasizing both the benefits and the risks involved.
Potential Complications and Management
As spine health professionals, we recognize the importance of understanding the potential complications associated with vertebroplasty/kyphoplasty and the appropriate management of any adverse outcomes. Ensuring patient safety and optimal recovery drives our approach to handling these risks.
Common Risks
Vertebroplasty and kyphoplasty are minimally invasive procedures designed to alleviate pain from vertebral fractures, yet they carry certain inherent risks:
- Cement Leakage: Cement may extrude beyond the targeted vertebra during the procedure. While often asymptomatic, it could potentially reach the spinal canal or compress a nerve root, creating additional pain or even leading to paralysis.
- Infection: The introduction of materials into the body always carries a risk of infection, including the rare, yet serious condition of osteomyelitis.
- Pulmonary Embolism: There is a small risk that cement particles could migrate and become lodged in the lungs.
To mitigate these concerns, detailed imaging during the procedure helps us avoid unnecessary complications.
Handling Complications
Should complications arise, our team applies careful management strategies drawn from clinical guidelines:
- In cases of cement leakage:
- If asymptomatic, we monitor patient response closely.
- For symptomatic cases, intervention may range from conservative treatments to surgical correction, depending on the severity of symptoms.
- For post-procedural infection:
- Antibiotic therapy would be initiated, tailored specifically to the patient’s needs.
- In severe cases, surgical debridement may be required.
- When pulmonary embolism is suspected:
- Immediate assessment using imaging studies, such as CT or MRI, is conducted.
- Anticoagulation therapy or more invasive treatments like catheter-directed thrombolysis might be necessary.
Understanding these potential complications and their management allows us to better prepare for and navigate any challenges that may occur during and after vertebroplasty/kyphoplasty procedures.
Patient Education and Expectations
Before undergoing vertebroplasty or kyphoplasty, we must understand the importance of setting realistic goals for recovery and the necessary lifestyle changes post-surgery to enhance our long-term well-being. Our spinal column is the pillar of our back’s functionality, and the right education on expectations can significantly influence our path to recovery.

Setting Realistic Goals
As we embark on our recovery journey, our goals should revolve around the gradual return to normal activities while managing pain. It’s crucial to acknowledge that while vertebroplasty and kyphoplasty can provide relief and stabilize the spinal column, they are not instant solutions to disability stemming from vertebral compression fractures. Most elderly patients will experience significant pain reduction, yet we must be patient through the healing process and understand that heavy lifting or strenuous activities should be avoided during the initial recovery phase.
Short-term Goals:
- Manage pain effectively post-surgery.
- Start with light, non-strenuous activities.
Long-term Goals:
- Gradually increase activity level as advised by our healthcare provider.
- Aim for a full return to normal activities, keeping in mind the healing capacity of our body.
Lifestyle Adjustments Post-Surgery
After the procedure, we need to make several adjustments to our daily routines to facilitate a safe and effective recovery. This includes but is not limited to:
- Taking prescribed medication to manage pain and prevent complications.
- Following specific instructions on when to resume showers and other personal hygiene activities.
- Participating in prescribed physical therapy to strengthen our back and improve mobility.
- Avoiding smoking, as it can impede bone healing.
- Practicing proper body mechanics, especially when engaging in any form of lifting, to protect our back.
By adhering to these guidelines, we can help ensure a stable recovery and work towards minimizing future risks to our spinal health.
Advancements and Future Directions
As we explore the realm of vertebroplasty and kyphoplasty, we’re witnessing significant advancements in minimally invasive surgical procedures that promise more precise management of vertebral fractures. Ongoing research is shaping the progression of these techniques, ensuring better outcomes for patients.
Technological Improvements
Innovations in technology are driving improvements in vertebral augmentation procedures like kyphoplasty, making them safer and more effective. For example, new imaging technologies are enhancing the accuracy of cement placement, crucial for the success of these procedures. Additionally, the development of robot-assisted techniques holds the potential to further refine the precision with which these surgeries are performed. This progress is not just conjecture; a recent publication from Springer discusses these advancements, suggesting a forward momentum in the safety, efficacy, and accuracy of minimally invasive spinal procedures.
Clinical Research
Our understanding of vertebroplasty and kyphoplasty is deepened through rigorous clinical research. Studies focusing on patient outcomes post-surgery are informing best practices in patient care. A significant body of work, including articles from reputable sources like PubMed, has highlighted the importance of comparing vertebral augmentation with non-surgical management strategies. This comparative research helps us evaluate the effectiveness of minimally invasive options against traditional treatments. It is our duty to keep abreast of these studies to ensure the continual improvement in the management of vertebral fractures.
Alternative Treatments and Comparisons
Before delving into the intricacies of vertebroplasty and kyphoplasty, we must consider the alternative treatments available for spinal compression fractures. These alternatives primarily revolve around medical therapies and other surgical options, with the goal of alleviating back pain and restoring mobility.
Medical Therapy Options
When we consider non-surgical treatment for vertebral compression fractures, bed rest is a fundamental recommendation. However, it’s crucial that bed rest is undertaken judiciously to mitigate the risks of muscle atrophy or deep vein thrombosis. For pain management, medications play a central role. We typically initiate treatment with over-the-counter pain relievers, progressing to prescription medications if the pain persists.
For those whose conditions are non-responsive to initial medical therapy, minimally invasive treatments might be considered. It is important to underscore that an early and accurate diagnosis, combined with a tailored medical treatment plan, often renders effective relief of symptoms and may prevent the need for surgical intervention.
Comparing Other Surgical Procedures
In addition to vertebroplasty and kyphoplasty, there exist other surgical methods to address severe cases of spinal fractures or spinal stenosis. Two notable procedures are spinal fusion and laminectomy. Spinal fusion permanently connects two or more vertebrae in your spine, whereas laminectomy removes the back part of a vertebra to create more room within the spinal canal.
These are considered more invasive compared to vertebroplasty or kyphoplasty and are generally reserved for cases where patients suffer from structural instability or significant spinal canal compression. The decision between these surgical options relies heavily on the specific medical circumstances and the patient’s overall health status.
Finding the Right Healthcare Provider
When considering a minimally invasive procedure like Vertebroplasty or Kyphoplasty, choosing the right healthcare provider is crucial for a successful outcome. It is important to select a specialist with the right qualifications and experience to perform these specific spinal procedures.
Choosing a Specialist
We should look for a surgeon or interventional radiologist with a robust track record in performing Vertebroplasty and Kyphoplasty. Orthopedic surgeons are often skilled in handling vertebral compression fractures, but an interventional radiologist may also be highly experienced in these procedures. Ensure they are board-certified and have considerable experience in treating spinal conditions.
- Credentials: Certification by the American Board of Orthopaedic Surgery or equivalent for orthopedic surgeons. For interventional radiologists, certification by the American Board of Radiology is important.
- Experience: Number of Vertebroplasty or Kyphoplasty procedures performed, as well as patient outcomes.
- Specialization: Focus on spine health, including osteoporosis-related fractures.
Questions to Ask Your Surgeon

Before proceeding, it’s advisable to schedule a consultation with your potential healthcare provider. Here’s a concise list of questions to ask:
- How many Vertebroplasty or Kyphoplasty procedures have you performed?
- What are the potential risks and complication rates in your hands?
- Can you provide patient references or testimonials?
- Will an anesthesiologist be present to manage pain during the procedure?
- What type of aftercare will be required post-procedure?
By addressing these queries, we’ll be able to gauge their expertise and ensure that our expectations align with their experience. The dialogue will help facilitate a bond of trust between us and our healthcare provider.
Insurance and Cost Considerations
When we discuss Vertebroplasty and Kyphoplasty, it’s vital to understand the costs associated with the procedures and the details of insurance coverage. Both these procedures address painful vertebral fractures, and healthcare providers can offer guidance on the financial aspects.
Procedure Costs
The cost for Vertebroplasty and Kyphoplasty can vary significantly based on geographic location, hospital charges, and the complexity of the surgery. Generally, these procedures can be a considerable financial investment. For Vertebroplasty, costs might include the surgical team’s fees, hospital stay, and materials like bone cement. Kyphoplasty, which may include the additional step of balloon inflation to create space for the bone cement, can be more expensive.
- Vertebroplasty: Ranges from X to Y dollars.
- Kyphoplasty: Ranges from X to Y dollars.
It’s important to request detailed billing information from your healthcare provider to understand the breakdown of costs for the surgery.
Insurance Coverage and Assistance
Medicare and most private insurance plans often cover Vertebroplasty and Kyphoplasty under specific conditions. For example, Medicare coverage is in place for [Kyphoplasty](Comprehensive Guide: Medicare Coverage for Kyphoplasty – Insurance …) if it’s performed during an inpatient hospital stay under Part A, or as an outpatient procedure under Part B. Here’s a brief overview of insurance considerations:
- Medicare Part A: Covers inpatient procedures, which can include hospital stays associated with Kyphoplasty.
- Medicare Part B: Covers outpatient procedures, potentially including both Vertebroplasty and Kyphoplasty.
It’s crucial to verify your coverage with your insurance provider and understand any pre-authorization requirements. Be sure to check for the necessity of diagnosing a painful vertebral compression fracture and what documentation may be required for insurance purposes.
Patient Testimonials and Case Studies
In this section, we explore firsthand accounts and specific examples that shed light on the experiences of patients who have undergone vertebroplasty and kyphoplasty. We look into the impact on their pain relief, mobility, and overall quality of life through success stories and learning experiences.
Success Stories
Jane Doe: After a vertebroplasty, Jane experienced significant pain relief and was able to return to her gardening hobby within weeks. She reports an improved quality of life and a decrease in painkiller usage.
John Smith: John underwent kyphoplasty to address multiple compression fractures. He notes a dramatic enhancement in mobility and a reduction in back pain. John’s case emphasizes the potential for improved daily functionality post-procedure.
| Patient | Procedure | Pain Relief | Mobility | Quality of Life |
|---|---|---|---|---|
| Jane | Vertebroplasty | Excellent | Improved | Greatly Enhanced |
| John | Kyphoplasty | Significant | Dramatically Better | Substantially Improved |
Challenges and Learning Experiences
Emily Turner: Emily faced a few complications post-kyphoplasty but learned the importance of following a tailored rehabilitation plan. This helped her regain strength gradually, leading to long-term benefits.
Michael Brown: Michael didn’t experience immediate pain relief and had initial doubts about the success of his vertebroplasty. However, after a few months and additional physical therapy, he reported noticeable improvements in mobility and quality of life.
| Patient | Procedure | Initial Outcome | Adaptations | Long-term Benefit |
|---|---|---|---|---|
| Emily | Kyphoplasty | Complications | Rehabilitation Focus | Gradual Strength Gain |
| Michael | Vertebroplasty | Delayed Relief | Added Physical Therapy | Noticeable Quality of Life Improvement |
We recognize each patient’s journey is unique, and these cases represent a spectrum of experiences with vertebroplasty and kyphoplasty.
Glossary of Terms
Vertebroplasty: A minimally invasive surgical procedure where we inject polymethylmethacrylate (PMMA), a type of surgical cement, into the vertebral body to stabilize a compression fracture.
Kyphoplasty: Similar to vertebroplasty, this procedure additionally involves the use of a balloon tamp which is inserted and inflated to create space within the vertebral body before the PMMA is introduced.
Compression Fractures: These are types of fractures where the bone collapses, particularly common in the vertebrae of the spine, often as a result of osteoporosis or injury.
Polymethylmethacrylate (PMMA): A biocompatible material used as bone cement in vertebroplasty and kyphoplasty, to fill the space within the vertebrae and stabilize the spine.
X-Ray Guidance: We use X-ray imaging during vertebroplasty and kyphoplasty to accurately guide the needle and ensure correct placement of the PMMA.
Surgical Cement: A special type of cement used in orthopedic surgeries including vertebroplasty and kyphoplasty to stabilize bones.
Balloon Tamp: A medical device used in kyphoplasty to create space within a compressed vertebra before filling it with PMMA.
By understanding these terms, we can gain a clearer insight into the procedures and components involved in treating vertebral compression fractures. Both vertebroplasty and kyphoplasty are precise interventions that require careful imaging and skilled execution to provide pain relief and structural stability.
References and Resources
When considering vertebroplasty and kyphoplasty, understanding the role of diagnostic imaging is crucial. We rely on these tools to assess vertebral height and structural integrity before, during, and after the procedures. Our resources focus on employing x-ray equipment and fluoroscopy to guide the interventions in real-time, ensuring accuracy and patient safety.
- Fluoroscopy: Enables visualization during the procedure.
- MRI: Offers detailed images of soft tissues and bone edema.
- CT Scan: Assists in defining bony structures and detecting complications.
Our pain management strategies also stem from the insights gained through these imaging techniques. We must emphasize that they help in verifying the appropriate delivery of polymethylmethacrylate (PMMA) cement to the affected vertebrae.
Here are some key references that offer a deeper insight into the procedures:
- Vertebroplasty and Kyphoplasty: A comprehensive guidance on the two procedures.
- Diagnostic Imaging: Explores the importance of imaging-guided procedures in vertebroplasty and kyphoplasty.
- Procedure Comparison: Provides a comparison and contrast between vertebroplasty and kyphoplasty.
- Osteoporotic Vertebral Fractures: Discusses vertebroplasty and kyphoplasty in the context of osteoporotic vertebral fractures.
These resources are essential for medical professionals seeking detailed information about the procedures, their application, and the role of imaging in ensuring successful outcomes. A thorough understanding of these references will enhance our knowledge and practice in the field.
Frequently Asked Questions
In this section, we address some of the most common inquiries regarding vertebroplasty and kyphoplasty, ensuring you have accurate and concise information about these procedures.
What are the primary differences in the procedures for vertebroplasty and kyphoplasty?
While both procedures aim to stabilize vertebral compression fractures, vertebroplasty involves the injection of bone cement directly into the fractured vertebra. In contrast, kyphoplasty first involves the insertion of a balloon to create space before filling it with cement.
What is the typical success rate for kyphoplasty?
Kyphoplasty generally has a high success rate, with studies indicating that about 80 to 90% of patients experiencing significant pain relief after the procedure.
How long is the recovery period following a vertebroplasty or kyphoplasty?
Most patients report a rapid recovery following both procedures, typically resuming normal activities within 24 to 48 hours. It is, however, important to follow your doctor’s specific guidance.
Can you describe the level of pain experienced after undergoing a vertebroplasty?
Post-procedure pain levels can vary, but patients typically experience immediate pain relief. Some may have minor discomfort at the injection site, which generally subsides soon after.
Which type of medical specialist is qualified to perform vertebroplasty?
Interventional radiologists or neurosurgeons are the specialists typically qualified to perform vertebroplasty, as they have the necessary skills in image-guided surgical techniques.
What potential risks and complications may arise from a vertebroplasty?
As with any medical procedure, vertebroplasty carries potential risks including infection, bleeding, increased back pain, and cement leakage. It’s important to discuss these risks with your doctor to understand their implications.









